Preventing substance abuse among adolescents. “Negative consequences of substance use”
Read also
Place of work: GKOU RO Orphanage No. 3 Taganrog
Modern society is characterized by an increase in the number of people using various types of drugs, which leads to an increase in the number of crimes. Particularly serious is the danger of a rapid increase in the number of minors using narcotic and toxic drugs.
According to statistics, 32% of teenagers resort to drugs as a way to avoid stress. 28% of teenagers try drugs for the first time (without much desire) under the influence of persons in authority for them, i.e. as a result of outside suggestion. 39.5% of teenagers try drugs out of curiosity.
Drugs have a depressing effect on all organs and tissues, and especially on the central nervous system.
The formation and development of drug addiction is characterized by the development of the following signs: mental, physical dependence and tolerance.
Mental dependence is a conscious or unconscious need to use a drug to relieve mental stress and achieve a state of mental comfort.
Physical dependence– a condition in which withdrawal syndrome develops in response to drug withdrawal. Occurs only in the presence of mental dependence.
Tolerance- this is the ability to tolerate toxic doses of a drug, resistance to a drug. An increase in tolerance is manifested in the fact that the initial doses of the drug do not cause the same euphoria, intoxication or other desired effect.
Most often, primary drug addiction is caused by age-related characteristics of the psychology of adolescents: the desire to establish themselves through a “special”, “interesting” pastime - unusual and risky. The main motives for this are: curiosity, imitation of leaders, submission, and sometimes protest against the norms of adult behavior. This usually happens in the absence of genuine, emotionally charged interests, spiritual values, skills for organizing leisure time, and clear positive social attitudes. Such personal and behavioral characteristics are precisely characteristic of adolescents who belong to the “risk group”. It is among them that adolescents with a certain readiness for drug addiction can be identified.
Factors contributing to drug addiction:
1. Social:- children from socially disadvantaged families, conditions of upbringing in the family (conflictful interactions between parents, lack of attention, control and authority of adults);
- unfavorable environment and social disorganization (areas characterized by high level crime, etc.);
- poor academic performance, lack of desire to continue studying at school;
- influence of an informal peer group;
- alienation and teenage rebellion (the teenager has no desire to go to school, feels “different” from everyone else, an outsider, and as a result, protest arises);
- initiation into drugs at an early age;
- tolerance public opinion to drunkenness, drug addiction, substance abuse.
2. Psychological:
- psychological and social immaturity of adolescents, infantilism, insufficient assimilation of social norms of behavior, constant excessive dependence on others, willingness to follow negative leaders, including readiness for criminal behavior;
- an increase in the number of children unable to adapt to the conditions of society;
- low resistance to mental overload, stress - reduced adaptability to difficult situations, conflict intolerance;
- severe tension, anxiety, self-doubt, low self-esteem, difficulties in communication;
- impulsiveness, in particular, with the desire to obtain pleasure, new sensations (pleasant and unpleasant), as quickly as possible and in any way.
3. Biological:
- inheritance by children from dysfunctional families of mental and biological features that contribute to the development of bad habits - drug use, alcohol, smoking;
- borderline neuropsychiatric disorders, mental retardation.
Consequences that drug addiction entails:
High mortality caused by drug overdoses, accidents while intoxicated, various diseases, frequent suicides among drug addicts;
- pronounced medical and social consequences drug use: mental disorders in the form of acute and chronic psychoses, pronounced personality changes up to its collapse, dementia, inability to work, etc.;
Criminal behavior of drug addicts due to changes in their personality; drug addicts commit crimes both for the purpose of acquiring drugs and in connection with severe mental disorders (psychoses) that have developed as a result of their use.
It is also necessary to take into account that recently drug addicts have been using more and more new substances that change their mental state. Thus, the number of cases of non-medical use of various medicinal drugs has increased, including often in combination with alcohol, as well as some drugs household chemicals.
Household and group forms of adolescent use of psychoactive substances are becoming more frequent. Groups are usually created by “informal leaders,” often adults who have experience using drugs and access to sources of drug acquisition.
Narcotic drugs and psychotropic substances are divided into 3 groups:
1. Drugs with sedative, analgesic and hypnotic effects - opium, morphine, heroin, noxiron (glutatemide), potent sleeping pills (barbamyl, sodium etaminal, etc.).
2. Exciting substances – caffeine, fanamine, etc.
3. Substances that cause hallucinations - hashish, cocaine, LSD, mescaline, etc.
The picture of drug intoxication is different, depending on the substance taken.
When intoxicated with drugs of the first group, pallor, dry skin of the face and body are noted, the pupils are sharply constricted, the pulse is rapid, outwardly such a person is lethargic, relaxed, and has a complacent mood.
If a drug addict has taken opium, morphine or codeine, then traces of “scratching” may be visible on the skin of the face, neck, and chest. When drugs are injected through a syringe, traces of injections into veins in various parts of the body are visible. In chronic drug addicts, the saphenous veins are poorly visible, have a whitish color, are hard to the touch, and along them there are scars from past inflammation at the injection sites.
When intoxicated with sleeping pills, also included in the first group, the face becomes red and sweaty. The intoxicated person is drowsy, spits or saliva drips from the corners of the lips, the eyes are shiny, the pupils are dilated, the gait is staggering, the fingers of outstretched hands are trembling violently. The speech is slurred, the words are indistinct, the drugged person does not finish them. At the same time, at first he is excited and easily becomes angry, rude, and cynical.
When intoxication ends, lethargy, a feeling of exhaustion, and irritability occur.
When intoxicated with substances of the second group, the leading symptoms are states of excitement, high mood, nervousness, loud laughter, fast sweeping gait, exaggerated gestures. At the same time, the face turns red, the eyes sparkle, the pace of speech is accelerated, the answers are quick, and obscene expressions are easily uttered.
At the end of intoxication, a feeling of fatigue, a feeling of weakness, increased drowsiness, and decreased mood develops. In this state, suicide attempts are possible.
When intoxicated by substances of the third group, the face is pale, the skin is dry, the eyes are shiny, the pupils are dilated, and the sclera is reddened. In cocaine addicts, the pupils are dilated, and the pallor of the skin of the back and wings of the nose stands out on the face.
Those who have smoked hashish seem lethargic, drowsy, and slightly stunned. This state can suddenly be replaced by an unreasonable challenge of fun, laughter, or vice versa, facial expressions of anxiety and fear appear with sudden movements to the side, imitation of the movements of people standing nearby. At these moments, the addict experiences pleasant (or unpleasant) “visions”, his consciousness is stupefied, and contact with him is difficult.
The state of people who have taken LSD most closely resembles the picture of acute psychosis, with influx of visual and auditory hallucinations and they are inaccessible to contact.
In addition to those listed, there is another type of drug addiction - mixed or polydrug addiction. Polydrug addiction is said to occur when a drug addict takes two or more drugs.
Withdrawal symptoms (“withdrawal”) develop in habitual drug addicts 5-12 hours after the cessation of the drug, they are somewhat reminiscent of the state of a severe hangover during alcoholism. This manifests itself in a feeling of malaise, lethargy, weakness, sweating, chills, pain throughout the body, a sad and, at the same time, angry-aggressive mood. At this time, the addict has only one desire - to quickly take the next dose of the drug. Most crimes are committed by drug addicts in this state. If he still cannot get the drug, the physical and mental condition of the drug addict worsens: loss of appetite, insomnia, vomiting, diarrhea, cramps, increased pain in muscles and joints - an extremely painful condition that drug addicts call “withdrawal.” At this time, hallucinatory-delusional experiences may occur. Withdrawal symptoms last up to 10-15 days, and then gradually decline. Providing specialized medical care softens the course of withdrawal, but still cannot eliminate it completely. Withdrawal is most pronounced when using opium, morphine, codeine, heroin and their derivatives. When using hashish or sleeping pills, it is weaker, but also difficult to tolerate.
You should pay attention to the following suspicious signs in the behavior and appearance of the child regarding the use of psychoactive drugs.
Signs of use of narcotic, psychotropic and other psychoactive substances:
· decreased interest in studies, academic performance, sports, absenteeism;
· increased need for money, loss of money and things from home;
· manifestations of deceit, avoidance of conversations under far-fetched pretexts;
· the teenager changed company, he made friends, whom he does not want to talk about, he tries not to even mention their names;
· the child returns from the street inappropriately cheerful or, on the contrary, inhibited, periods of unmotivated irritability or aggressiveness have appeared;
· instability of attention, memory impairment, thinking disorders, delusional statements;
· comes home with the smell of alcohol, or the smell of acetone emanates from clothes and hair, or the smell of burnt plastic from fingers;
· glue stains appeared on clothes;
· scratches appeared on the hands, traces of minor burns, traces of injections in the projection of the veins on the forearms, the back of the hands, bruises; the teenager tries to wear long sleeves, even if it is out of season;
· there is skin irritation in the area of the nasolabial triangle;
· when returning home, the pupils of the child’s eyes are sharply dilated or narrowed to points, “unseeing gaze”;
· “red” sclera (dilated vessels of the conjunctiva of the eyes);
· when looking to the side, the eyeballs make pendulum-like movements;
· there is a violation of fine coordination movements;
· the rate of speech is changed (slow or accelerated), speech is inarticulate;
· unreasonable decrease or significant increase in appetite, complaints of a metallic taste in the mouth;
· bags, matchboxes with crushed mixture or tablets, syringes, acetone, pieces of bandage or gauze soaked in liquid with a brownish tint, smoked spoons, thimbles appeared in the child’s things.
If the above signs are detected, it is necessary to urgently consult a minor with a psychiatrist-narcologist. Only a specialist can determine which psychoactive substance a minor is using.
Consequences of smoking marijuana:
Use – memory impairment, decreased attention, perception and thinking ability. Slowing reflexes and decreasing motor activity.
Systematic use – development of diseases respiratory system, lung cancer and the development of malignant brain tumors, damage to the immune system and the development of impotence.
Consequences of using ecstasy
Use – distorted perception of reality, hallucinations, severe dehydration, nausea, convulsions, apathy and depression.
Systematic use – destruction of the liver, kidneys, impotence, mental disorders, cardiovascular failure.
Consequences of heroin use
Use – distorted perception of reality, dizziness, increased urination, nausea, vomiting, sweating, inadequate speech perception, “clown mask” on the face.
Systematic use – scarring and compression of veins as a result of injections, liver and kidney disease, physical and psychological wear and tear of the body.
Overdose – low arterial pressure, slow and irregular heartbeat, low temperature body, deep sleep, stupor (immobility), coma, death.
Consequences of cocaine use
Use – distorted perception of reality, anxiety, increased heart rate, loss of appetite, increased activity and fatigue, nervous tremors, nausea, vomiting, increased body temperature.
Systematic use – excessive nervousness, frequent unreasonable mood swings, hallucinations, impotence, cardiac arrhythmia, chest pain.
Overdose – delirium, rapid, disturbed shallow breathing, loss of consciousness, death.
Consequences of using methamphetamines
Use – frequent dizziness, dry mouth, frequent urination, diarrhea, hallucinations, fainting, fever.
Systematic use – chronic sleep problems, anxiety and tension, high blood pressure, rashes, paranoia, delusional syndromes.
Overdose – fever, coma, cerebral hemorrhage, death.
1.1. BASIC CONCEPTS AND TYPES OF PSYCHOACTIVE SUBSTANCES
There are various approaches that define the basic concepts of the prevention of substance use. In some cases, the concept of “drug” is defined as a key term and actually refers to various psychoactive substances . However, we will assume that drugs belong to one of the types of surfactants.
The concept of surfactants is basic in legislative documents regulating the organization of activities in the field of preventing the use of surfactants in the educational environment . The main documents of this kind include the “Concept for the Prevention of Substance Abuse in the Educational Environment.” The contents of this document are presented in Appendix 1. The concept of prevention outlined in it has been very seriously “developed” and provides the necessary guidelines for specialists in the field of school prevention of the use of psychoactive substances.
So, the basic concept of the sphere of prevention of the use of surfactants is psychoactive substance.
Psychoactive substances -natural and synthetic substances that change the human condition. These substances, entering the human body, change his mental and physiological state. At the same time, a person’s behavior, perception of the environment, mood, cognitive ability and motor functions may change. .
There is a wide variety of surfactants. Some surfactants are used for medical purposes as painkillers and sleeping pills. In sports, surfactants are associated with the concept of “doping”. IN ordinary life we also encounter the consumption of surfactants when we drink coffee or tea. However, the use of some surfactants can lead to very tragic consequences for human health. Of course, the greatest danger among surfactants is narcotics. .
If we talk about surfactants in general, they are neither good nor bad. The degree of their “harm/benefit” depends on who, how and for what purpose uses them . There is no doubt that surfactants should be distinguished according to the degree of their effect on the body. Drinking tea or coffee does not have any dangerous consequences for humans. These drinks are consumed by many people in different countries of the world without any particular harm to health. However, the use of some of the surfactants can lead to serious illnesses.
The most dangerous to the health of schoolchildren are: tobacco, alcohol, drugs and inhalants. When organizing activities in the field of school prevention of psychoactive substance use, we must strive to reduce the likelihood of schoolchildren introducing these psychoactive substances.
In the future, the concept of surfactants in the manual will be understood primarily as these 4 types of psychoactive substances: tobacco, alcohol, drugs and inhalants. In this paragraph we will give definitions of each of them.
There are various classifications of surfactant types. We will focus on two of them.
Natural and synthetic psychoactive substances
First, let's list some of the most common natural Surfactant
Marijuana – collective term for dried leaves various types hemp. Smoking marijuana is more dangerous than smoking tobacco .
Cocaine– white fine crystalline powder obtained by extraction from the leaves of the coca plant . This shrub grows in South America. Coca leaves are a potent mental stimulant.
About synthetic surfactants. Unfortunately, despite criminal penalties, the drug business is thriving in our country. This is due to its high profitability. Therefore, in addition to natural surfactants, a wide variety of synthetic surfactants are also supplied to the “drug market”. Let's just talk about heroin - one of the most famous and dangerous synthetic drugs.
Heroin –synthetic drug. By the look White powder. Heroin is smoked, swallowed, snorted, or injected. When you take it, you feel drowsiness, warmth, and a surge of strength and spirit. This drug is dangerous due to overdoses and the rapid onset of strong and difficult to overcome addiction. .
Legal and illegal psychoactive substances
Let's take a closer look at this classification.
Legal surfactants – psychoactive substances not prohibited by law for use, storage and distribution . The most famous legal surfactants: nicotine, caffeine and alcohol.
Nicotine. Contained in tobacco, cigarettes, cigarettes, cigars, shag, etc. The use of nicotine in any dose is dangerous to human health. The most developed countries sharply restrict trade in tobacco products and ban smoking in all in public places and at work.
Caffeine. Caffeine is found in tea, coffee and chocolate. It has a stimulating effect on the central nervous system. Frequent and copious consumption of strong tea or coffee can harm the body.
Alcohol – any drink containing the toxic substance ethanol (ethyl alcohol). Alcohol in small quantities acts on the body as a stimulant. In moderate and large doses, alcohol inhibits the body's activity. Alcohol is found in beer, wine, spirits, some medicines, syrups and perfumes. Long-term alcohol abuse can cause chronic disease alcoholism .
Legal surfactants are used openly by adults. And these actions do not cause legal liability. However, the consumption of some legal surfactants (tobacco and alcohol) can lead to significant destruction of human health.
Observation practice
At parent meetings devoted to the topic “Prevention of the use of surfactants,” one should not say that “alcohol in small quantities acts on the body as a stimulant.” In the Russian mentality there is such a feature as “lack of a sense of proportion.” Such an objective determination of the properties of alcohol (for small doses) can push people who drink alcohol to a position of “self-justification”, and therefore, to the risk of excessive consumption of alcoholic beverages.
Preventologist position
Each adult is responsible for his own health and the consequences that arise from consuming alcohol and tobacco;
Parents must remember: regardless of their wishes, the behavior of parents is a role model;
Schoolchildren should know that the use of tobacco and even small doses of alcohol is harmful and dangerous for them.
Illegal psychoactive substances
Illegal surfactants include drugs. They are prohibited by law for production, transportation, storage, sale and consumption. Drug use affects a person’s psyche in such a way that he is unable to live a full life. An addict cannot make sound decisions, control his behavior, or work productively.
In our opinion, intermediate position between legal and illegal Surfactants are occupied by inhalants.
Inhalants(from English inhalation - inhalation) - chemical substances technical and household chemicals. We are talking about gasoline, acetone, various aerosols, cleaning liquids, adhesives, paints, paint solvents, nail polish remover, lighter gas, etc.
Inhalants are also called “volatile substances” because they actively evaporate. Another possible name for inhalants is toxicants. We will discuss in more detail about inhalants and their effect on the body in the second chapter.
We will also designate other concepts that are significant for the sphere of prevention of surfactant use (hereinafter, prevention of surfactants).
Protective factors – various factors, reducing the likelihood of surfactants. Protective factors increase people's intention not to use substances. Every person has great protective capabilities for health. External and internal protective factors can be distinguished. For example, internal protective factors include: adequate self-esteem, decision-making skills, communication skills, etc.
External protective factors: family support, training at a valeological school, etc. .
Risk factors -factors that increase the likelihood of using psychoactive substances. There are many risk factors. For example, the availability of drugs, growing up in an “alcoholic” family, etc.
Prevention target - object to which work is aimed at preventing the use of surfactants. In the field of prevention of URAS, the following targets are distinguished: individual, family, peer group, school, society.
Substance addiction – the state of a person when he constantly uses any surfactant and cannot stop.
In the course of further presentation of the material, other important concepts in the field of prevention of surfactants will be defined.
1.2. THE PROBLEM OF PSYCHOACTIVE SUBSTANCE USE
SUBSTANCES IN TEENAGERS AND ITS SOLUTION
Numerous studies indicate a significant increase in the consumption of surfactants that has occurred in our country over the past two decades.
During this time, the problem of drug addiction has worsened to the greatest extent. At the beginning of the 21st century, according to official data, from 2 to 3 million drug addicts were registered in Russia. According to experts, the real number of drug addicts in the Russian Federation is 2-3 times higher and it continues to grow. The approximate life expectancy of drug addicts from the moment they start using drugs is on average 4 to 5 years.
In Russia, as throughout the world, young people under the age of 30 predominate among drug users. The growth rate of drug addiction in this age category is the highest. It is known that 20% total number drug addicts in Russia are schoolchildren, 60% are young people aged 16–30 years, and only 20% are older people.
In the field of drug consumption over the past 15 years, the following trends can be identified:
1) Russia has one of the highest levels in the world dynamics of drug use. There are countries in Europe where per capita they consume individual species There are more drugs than in the Russian Federation. For example, on marijuana. However, in general, the dynamics of drug consumption in the Russian Federation is one of the highest in the world.
2) In the structure of drug consumption, drug consumption begins to take first place heroin. Heroin is one of the most dangerous drugs for health. We briefly mentioned it in paragraph 1.1. Russian peculiarity heroin consumption is that it is most often used in large cities.
3) Rejuvenation of surfactant consumers. Drug use is growing especially rapidly among teenagers. The average age of initiation into drugs is constantly decreasing and by 2012 it was 13 years old. Therefore, it is no coincidence that the problem of drug addiction is referred to as “teenage”.
The arsenal of surfactants consumed by teenagers is large – from medicines, used for the purpose of intoxication (diphenhydramine, pentalgin, cyclodol, etc.) into illegal drugs.
Alcohol consumers are rejuvenating in our country. As a rule, the first samples of alcohol occur at the age of 9-10, and regular initiation begins at the age of 12-13. According to our data, the number of schoolchildren in Izhevsk who have experience of “trying” alcohol increases with age (from 18% in the 3rd grade to 40 in the seventh).
Over the past 20 years, sampling and occasional drinking have become normative behavior for teenagers. According to Arefyev A.L., 82% of adolescents and youth aged 12-22 years drink alcohol.
Since the second half of the 90s of the last century, adolescents aged 12-14 years old with a diagnosis of substance abuse. Subsequently, there is an increase in the number of drug addicts and their rejuvenation. Substance abuse can lead to serious health problems. There are many cases where the consumption of inhalants led to death.
According to Rospotrebnadzor, more than half of the population in Russia smokes. If there is a reduction in the number of smokers in the world, then in our country the opposite is happening. In the Russian Federation from diseases associated with smoking, from 330 to 500 thousand people die annually. Nowadays, some children start smoking at the age of eight.
The head of the National Health League, academician Leo Bokeria, comments on the situation: “We have one of the highest levels of tobacco smoking in the world. 28% of the world's population smoke tobacco, in Russia 60.4% of men smoke; 25.5% women; 33% of secondary school students. The average number of years of life lost when dying from smoking-related diseases is 19 years for men and 16 years for women. This is a huge wasted part of life. And this cannot be tolerated!” .
Previous use of tobacco, alcohol and inhalants increases the risk of drug use. In particular, previous alcohol consumption by children and adolescents actively helps prepare the body for drug use. Up to 75% of alcoholics and drug addicts began using psychoactive substances as teenagers.
Preventologist position
Addiction to drugs in adolescents, as a rule, develops (if it develops) along the line tobacco - alcohol - marijuana - drugs. Numerous studies show that the earlier a person starts using tobacco or alcohol, the higher the risk that he will turn to drugs. Thus, by preventing smoking and drinking alcohol among schoolchildren, we are pursuing a long-term goal - preventing drug use.
The increase in the consumption of psychoactive substances by children and adolescents has updated activities in the field of preventing tobacco smoking, alcoholism, drug addiction and substance abuse. Over the past 10 years, the situation in the field of prevention of surfactants has changed. A theoretical and research base has emerged. The objectives of preventive activities were formulated, the directions and principles for constructing preventive programs were determined. Legislative documents have appeared that make it possible to develop and implement programs for the prevention of surfactants at different levels.
Actively and effectively operating charitable organizations have appeared in the field of prevention of chemical surfactants. However, there is still no good coordination of the work of government and public organizations.
Situation in the system general education is such that only less than 10% of schoolchildren can be considered healthy, and their health deteriorates from the first to the graduating class.
It should be noted that in recent years, work has been more actively developed in the field of school prevention of accidents. In fact, over the last 10 years the school has taken responsibility for the health of students.
Currently, the secondary school is becoming the central link in the system dealing with the primary prevention of psychoactive substance use. For example, almost every school in Izhevsk, to one degree or another, implements programs for the prevention of chemical surfactants. This is a completely logical and adequate reaction to the threat of teenage drug use.
It can be stated that over the past 10 years the state and society have moved to a position of active practical actions in the field of prevention of surfactants. However, the efforts made are not enough, since the increase in the consumption of surfactants among children, adolescents and young people continues.
Observation practice
Despite a number of positive changes, the prevention of accidents in schools is still “resting” on the enthusiasm of individual teachers and school leaders. You shouldn't exploit their enthusiasm endlessly. The best school preventive specialists, who work effectively and have their own preventive programs, should be supported in every possible way (including financially).
The problem of reducing the consumption of tobacco, alcohol, toxicants and drugs by children and adolescents is multidisciplinary in nature, which means that it is necessary to take into account many of its aspects (personal, social, medical, family, law enforcement, etc.). This requires an interdepartmental approach to solving it.
Prevention of surfactants should not be reduced to a set of events, campaigns and individual programs. If we want to achieve sustainable and thorough results, it must become an area long-term activities based on theoretical approaches and program activities of trained professionals. Moreover, this activity should be aimed at all prevention targets: individual, family, peer group, school and community.
Currently, there is no unified conceptual approach to the prevention of surfactants at the state level. We are talking about an approach that combines the efforts of departments, public organizations, educational institutions and citizens in solving an extremely important task for our state - the task of reducing the consumption of tobacco, alcohol, inhalants and drugs by adolescents.
1.3. PREVENTION OF PSYCHOACTIVE SUBSTANCE USE: CONCEPTS, CLASSIFICATIONS, LEVELS, GOALS AND OBJECTIVES
Concept n rophylaxis comes from the Greek word prophylactic, which means protective. It is interpreted as follows: prevention – system of measures to prevent diseases, preserve health and prolong human life .
Prevention aims to improve the quality of life. The quality of life is largely determined by the level of human health. In turn, s health - This harmonious combination physical, mental and social well-being of a person .
The manual deals with prevention in a narrower sense, namely, the prevention of the use of surfactants.
Prevention of surfactants - activities aimed at preventing the use of surfactants.
In the 70s of the 20th century, the World Health Organization (hereinafter referred to as WHO) proposed a classification of types of prevention, which is now the most common in Russia. She distinguishes between primary, secondary and tertiary prevention of surfactant use.
Primary prevention - a set of measures aimed at preventing the use of surfactants. Primary prevention is carried out among children and adolescents who have no experience of consuming surfactants. Her goal: prevention of surfactant use. The following options for setting goals are also quite legitimate: 1) Delay the start of using psychoactive substances by children and adolescents; 2) Reduce the likelihood of using surfactants.
The main objectives of primary prevention: 1) the formation of personal responsibility for one’s health; 2) developing skills that reduce the risk of consuming surfactants.
Preventologist position
It is fundamentally important to begin primary prevention of surfactants before the age of the first samples. That is, preventive work in secondary schools should be carried out from the first grade. There are several reasons for this. Firstly, prevention is much more effective among those who do not yet use psychoactive substances. Secondly, initiation into any surfactants begins with alcohol and tobacco. It is alcohol and tobacco that are the “gateway” substances. Preventing their use helps prevent drug use.
Secondary prevention - a set of measures aimed at working with the “at-risk group”" Secondary prevention is carried out with persons who already use surfactants. However, they are not yet chemically dependent people and do not need special treatment. Most often, the “risk group” includes teenagers and young people. In recent years, the number of adolescents at risk has increased. This means that the need to develop and implement secondary prevention programs has increased.
Tertiary prevention - a set of measures aimed at working with chemically dependent people in order to prevent breakdowns and relapses of the disease. The term “chemically dependent people” will be discussed in more detail in paragraph 2.1.
The possibilities of tertiary prevention are much lower than those of primary and secondary prevention. This type of prevention, organized in government medical institutions relies mainly on medical influence. However, the existing treatment methods are ineffective. Statistics from drug treatment centers and rehabilitation programs around the world provide a disappointing figure - about 90% of all drug addicts who have undergone detoxification in any treatment centers return to taking drugs. It is clear that maximum efforts should be directed towards primary and secondary prevention.
In the last two decades, new models of tertiary prevention have emerged that rely more heavily on psychotherapeutic and religious approaches. We are talking about the so-called anti-drug non-profit organizations (hereinafter, ANNCO).
ANNCOs do not engage in medical rehabilitation. They provide social rehabilitation services. Such ANNKO centers today make up at least 90% of all rehabilitation institutions in the country. The effectiveness of ANNKO social rehabilitation programs is from 40 to 60%.
Along with the above classification of types of prevention, in recent years another one has begun to be used in our country. This classification highlights universal, selective and indication-based prevention.
This classification is presented in more detail in Table 1 “Three types of prevention”.
Table 1
Three types of prevention
| Base | Universal | Electoral | According to indications |
| Goal of prevention | Prevention of surfactant use | Prevention of substance abuse | Contain the progressive development of substance abuse |
| Prevention target | Population as a whole | The risk group as a whole. For example, children of alcoholics | People with chemical dependency |
| Selection of participants | Participants are not selected | Participants are invited | Participants are selected strictly according to indications |
| Requirement for a specialist | Can be with anyone basic education | Experienced specialists | Special training for experienced personnel |
| Price | Low | Above universal programs | Most expensive |
There are other classifications of types of prevention. For example, they distinguish nonspecific And specific prevention.
Nonspecific prevention can be defined as indirect, since it does not directly address the problem of substance use. For example, non-specific prevention measures include: installing locks on entrance doors, insulating basements and attics, etc. Other common examples of nonspecific prevention: organizing leisure time for children and adolescents, activities of youth centers, sport competitions. This approach to prevention creates an alternative to the use of psychoactive substances for adolescents and young people and organizes their employment in their free time.
Activities within specific prevention focuses on a target group. Such prevention includes: training in preventive programs, conducting psychological training for teenagers on the topic “Be able to say no,” psychology lessons on preventive topics, publishing specialized literature, etc.
Also distinguished levels prevention: personal, family and social .
Work for personal level is aimed at the formation of certain personality qualities, which we previously defined as “protective factors”. The most important of them are: communication skills, self-confidence, stress resistance, pressure resistance and decision-making skills. A common form of preventive classes for the personal level: trainings and group training .
Family level involves influencing the family. Forms of conducting classes for this level: thematic parent-teacher meetings, trainings, family consultations, involvement of parents in school prevention programs for AFVs.
Social level is aimed at changing social norms regarding the use of psychoactive substances, as well as changing attitudes towards consumers in society. This level of prevention helps create favorable conditions for preventive work at the personal and family levels. Forms of work for this level: social advertisement, training seminars for specialists in the field of prevention.
The introduction of people to surfactants is a probabilistic process and it is caused by a combination of various circumstances and factors. The general goal for primary, secondary and tertiary prevention of AAS can be formulated as follows: reducing the likelihood of using surfactants.
The following goal setting is also quite legitimate: creating conditions for participants in preventive programs to understand their own behavior patterns, develop personal resources and strategies in order to adapt to environmental requirements or change maladaptive forms of behavior into adaptive ones.
Based on various sources, in the field of prevention of surfactants among children and adolescents, we can highlight the following most important tasks:
Contribute to increasing the knowledge of adolescents and young people by discussing problems related to psychoactive substances;
Change value attitude children and youth to surfactants;
Form personal responsibility for your health;
Promote awareness of your own goals and ways to achieve them;
Build personal resources that reduce the likelihood of using psychoactive substances.
1.4. FEATURES OF ADOLESCENCE
In the last 15-20 years, there has been an unfavorable trend towards rejuvenation of surfactant consumers. Using tobacco and alcohol, trying inhalants and drugs usually begins in adolescence. Unfortunately, in recent years, cases have become more frequent when the “first attempts” of tobacco, alcohol and inhalants occur in childhood.
The characteristics of adolescence (primarily from 13 to 15 years) suggest that this age period in itself is a risk factor for the consumption of psychoactive substances. Let us highlight those age-related characteristics of adolescents that are most likely to provoke the use of psychoactive substances.
· The presence of internal contradictions and doubts. Many studies also suggest that many older teenagers have high anxiety and low self-esteem. According to I. Kon, the formation of self-awareness is the central process of early adolescence. An incompletely conscious “I” “pushes” adolescents toward unconscious anxiety. Anxiety is also associated with rapid physical and sexual maturation, as well as the presence of internal contradictions. Teenagers with increased anxiety and depression may use alcohol to improve their well-being, to relax and feel more confident. In some cases, alcohol consumption by teenagers is their reaction to feelings of anxiety and loneliness. Alcohol allows them to get rid of self-doubt, shyness, anxiety for a certain time and overcome social prohibitions. Research has shown that adolescents who abuse alcohol experience feelings of self-dissatisfaction.
· Conflict. Older teenagers themselves often note that they are characterized by high levels of conflict. Indeed, many of them are characterized by rudeness and stubbornness. In early adolescence, teenagers move away from their parents. This circumstance increases the risk of conflicts with parents and manifestations of disrespect towards them. In many cases, “the relationship between children and parents is asymmetrical and unequal. Many parents, accustomed to controlling their children, are painfully aware of the weakening of their power.” The emancipation reaction reflects the contradictory aspirations of the teenager. Due to their inexperience, adolescents need help and support from adult specialists. However, they do not always turn to an adult for advice and help. In itself, turning to an adult is internally conflicting for them - they feel weak in comparison with him. Frequent consumption of alcohol in order to relax and relieve psychological stress indicates the existence of serious personal problems. Despite their desire for independence, teenagers are not completely confident in their abilities. The teenager overly actively defends his point of view not because he considers his statements to be true, but only because it is his opinion. It is important for him to defend it. Obvious manifestations of the emancipation reaction consist of open disobedience, ignoring the demands of parents or teachers, other adults. All attempts by adults to control a teenager’s behavior, to impose their views, interests, and petty supervision on him usually cause pronounced resistance. As a sign of protest against the dictates of their parents, a son or daughter can do everything “out of spite”: skip classes, smoke, etc. In more acute situations, teenagers run away from home and start using alcohol, drugs and toxic substances. Surveys of teenagers who abuse alcohol showed that they perceive alcohol consumption as a “form of protest.”
· The desire to learn new things. The desire of teenagers to learn everything new and unusual is understandable. They want to quickly become adults and adopt the habits and ways of behavior of their elders. Such motivation of adolescents in an unfavorable situation leads the teenager to use psychoactive substances. A normally developing teenager is always passionate about something: technology, sports, music, drawing, some branch of science. These hobbies can change, or they can be stable, turning into activities at a professional level. However, not all teenagers have socially useful, meaningful hobbies. Research has shown that 58% of teenagers do not have such hobbies, but are content with entertaining leisure activities. This is especially evident in “at-risk” adolescents. Research has shown that 79% of adolescents and young men who occasionally use psychoactive substances do not know how to occupy themselves with something specific and useful. Apart from a tendency to primitive groupings with peers, they have no interests.
· Need for informal communication with peers. Informal communication is the leading type of communication for older teenagers. The grouping reaction is especially pronounced at this age. In the street microenvironment, a teenager can gain a high social and personal status. This is especially important if he does not find any real field for self-affirmation in any other place (family, school, etc.). In a group, a teenager satisfies the need for free, unregulated communication, where he finds a means for self-expression. It is known that adolescents who are rejected and isolated in the classroom are forced to look for other peer groups to satisfy the needs of the developing personality for recognition. They come into confrontation with the class team and rely on the support of “street companies.” In most informal teenage groups, there is a strict hierarchy and subordination to leaders. Drinking alcohol in groups often plays the role of a kind of initiation into group membership. Drinking alcohol is becoming a typical activity for many antisocial groups. Since the number of antisocial informal youth groups has now increased, the growth of teenage alcoholism also becomes understandable.
· Feeling of adulthood. L.S. Vygotsky considered the main new formation of adolescence to be “the feeling of adulthood.” Older teenagers gradually separate from their parents and acquire independent living skills. Drinking alcohol is often perceived by them as a manifestation of adulthood, and being intoxicated allows them to become more independent. In fact, drinking alcohol for them is an element of experimenting with different styles of adult behavior. The desire to be an adult encourages a teenager to behave on the edge of what is permitted and forbidden, testing the “strength” of the norms, laws, and traditions of society. For a significant portion of older teenagers, drinking alcohol becomes a kind of ritual rite of passage into the adult world. Drinking alcohol is an important part of the role adults are so eager to play. Studying life path adolescents using psychoactive substances showed that they all faced the situation of the impossibility of satisfying their actual, vital social needs, including age-related ones.
As a summary for the paragraph, we can say that in late adolescence there are many risk factors that increase the likelihood of using psychoactive substances. This situation is aggravated by instability in social, economic and other spheres of life. In these conditions, the state, family, educational and public organizations, and other social institutions should build an effective system of working with older adolescents, which will reduce the risks of their involvement in substance abuse.
1.5. REASONS FOR PSYCHOACTIVE SUBSTANCE USE IN ADOLESCENTS
The reasons why teenagers start using psychoactive substances are varied. Let's highlight the most important of them.
Age specifics. One of the characteristics of adolescents is exaggerated ideas about their own physical capabilities and inadequate optimism regarding health in the future. That is why they are of little interest in the dangerous health consequences of using surfactants and the numerous warnings from adults.
Evolving Mindset. A teenager's thinking becomes more flexible and abstract. It allows you to consider logical alternatives to behavior and the possibility of deviation from the rules. Teenagers may notice the contradictory behavior of adults. They can formulate statements that are the opposite of what adults instill in them. They look for counter-arguments and rationalize why they ignore sound and healthy information. This undermines the knowledge they previously acquired about the dangers of using surfactants. Health issues, overshadowed by immediate social interests and needs that are relevant to them, fade into the background.
Peer pressure. Parental influence decreases with age, while peer pressure increases. It is known that informal communication is the leading type of communication among adolescents. A teenager’s communication with a peer group often contributes to the use of psychoactive substances. The stronger the connection with the group, the more the individual is influenced. More amenable to the group are anxious teenagers with low self-esteem.
Family Features. If there are people in the family who use psychoactive substances, then the risk of becoming involved with them increases.
A television. The use of surfactants is often shown on screens. Teenagers may have the idea that the use of psychoactive substances is the norm of life. Some teenagers imitate “screen heroes.”
Knowledge, attitudes, expectations. Insufficient knowledge and a positive attitude towards the use of psychoactive substances contribute to their initiation into them.
Psychological traits. The use of surfactants is also associated with certain psychological qualities. First of all, with the following traits: low self-esteem, undeveloped communication skills, increased need for social approval, anxiety, inability to withstand pressure and cope with stress. The presence of these traits increases the risk of addiction to substance abuse.
Department of youth policy The Ministry of Education of the Russian Federation conducted a large-scale study among adolescents and young people to determine the level of drug use among adolescents and young people. The following characteristic features of drug users were identified: lack of compassion for people, extreme degree of selfishness and greed.
Pharmacological properties of surfactants. All surfactants are addictive to varying degrees (addiction). Therefore, having started using psychoactive substances for social or psychological reasons, a teenager may continue to use it over time due to a physiological need. Over time, tolerance to surfactants develops and the body requires increasing doses. Stopping surfactants causes pain withdrawal syndrome. Thus, the pharmacological properties of surfactants contribute to their regular use.
Self-medication, overcoming stress. Some teenagers with increased anxiety, low mood and depression use psychoactive substances to improve their well-being. This allows them to relax and feel more confident.
Deviant behavior. Experts believe that the use of psychoactive substances is part of the deviant behavior syndrome. It is characterized by a special lifestyle and values. It manifests itself in the use of surfactants. Such teenagers usually study poorly, do not play sports, do not attend additional education centers, lie, and engage in petty theft and fraud. The concept of deviant behavior will be discussed in the next paragraph.
There is also a point of view that drug addiction is formed due to the following reasons:
· social immaturity, when a person gives in to curiosity and does not think about the consequences of using surfactants;
· personal experiences and problems;
· influence of unhealthy environment;
· the desire to follow “fashion” and the desire to imitate;
· psychological stress in the family.
· propagation of pseudoculture and lack of spirituality;
· feeling of “herdness”;
· the desire to appear strong, courageous and original in front of the opposite sex;
· orientation towards consumerism and entertainment;
· lack of awareness-raising work, preventive measures and active methods to combat the abuse of psychoactive substances.
1.6. SCIENTIFIC THEORIES
The use of surfactants is considered by many scientific theories. Based on their analysis, we can conclude that the use of surfactants is caused by many factors, among which there is no main one. None of the theories alone can fully explain such a complex phenomenon as the use of surfactants.
In recent decades, theories have emerged that describe the interaction of cognitive and emotional, social and personal factors in the use of psychoactive substances.
Let's get acquainted with two well-known theories that are often used to develop school programs prevention of surfactants. These are Bandura's theory of social learning and Jessore's theory of deviant behavior. They represent a popular conceptual approach called life skills building. We will talk about it in more detail in paragraph 4.2.
Preventologist position
The introduction of children and adolescents to the use of psychoactive substances is a probabilistic process that depends on the confluence of a large number of circumstances. The process of communion is associated with two phenomena .
The first is the presence of certain inclinations, traits, properties and qualities of the person himself, including genetic, physiological, psychological, social and moral. These qualities determine the demand for surfactants.
The second is the availability of surfactants in society. Availability is closely related to surfactant offerings. Preventing addiction to surfactants involves a combination of measures to reduce the demand for and supply of surfactants.
Bandura's theory
The theory is that children learn adult behavior through imitation of adults (by observing them) and positive reinforcement of acceptable behavior. If a child sees famous people who use surfactants, he strives to imitate them. He can imitate “TV heroes” and real people. By observing a group of older teenagers using tobacco or alcohol, children develop the belief that this is normal behavior. They may believe that this behavior makes them more mature and “cool.”
Bandura's theory places great importance on self-regulation and self-control. This is because susceptibility to social influences depends on the child’s attitudes and beliefs. Children facing serious life goals Those who are not compatible with the use of tobacco and alcohol will most likely not “succumb to harmful influences” and will refuse to use surfactants.
From the point of view of Bandura's theory, susceptibility to social influences is primarily due to:
Low self-esteem;
Self-doubt;
Dissatisfaction with oneself;
Increased need for social approval;
Inability to control oneself;
Inability to defend your point of view.
According to this theory, resistance to social influences can be nurtured (formed). The purpose of such education: the formation of psychological immunity to harmful social influences, in our case – to the use of surfactants.
Jessore's theory
This theory has another name - theory of deviant behavior(hereinafter referred to as OP). As a rule, OP manifests itself in adolescence. Manifestations of OP in adolescence include: use of psychoactive substances, early sexual activity, minor offenses, truancy from school, etc.
The OP serves an important purpose for some teenagers required function. For example, smoking and drinking alcohol allows them to appear interesting and independent. OP can also help overcome boredom, anxiety or social isolation. For those who study poorly, EP serves as a way to increase self-esteem and achieve a certain social status. With low academic performance, adolescents’ self-esteem falls and to restore it to an acceptable level for the individual, substance abuse is often used in an informal peer group. Thus, OP becomes a means of overcoming failure.
Anxious teenagers who do not have the skills to cope with stress and do not know how to interact with other people are at greatest risk of OP. Difficulties in interpersonal relationships and the associated psychological discomfort give rise to behavioral deviations. It would be naive to believe that in these circumstances an explanation of how harmful surfactants are to health is sufficient. For the troubled teenager interpersonal interaction, knowledge about the dangers of surfactants is irrelevant.
Teenagers begin to use psychoactive substances when they cannot satisfy their basic needs. What worries a teenager first of all? Let us designate the basic needs of a teenager through such components of personality as:
- I-physical;
- Self-social;
- I am sexual;
- I am psychological.
Self-physical. It is known that during adolescence, body shape changes significantly and rapid growth occurs. Moreover, physically, adolescents develop unevenly. H. Remschmidt notes: “Young people have a poor understanding of variability physical development; minor, imaginary deviations from the norm serve as a reason for exaggerated fears. Considering that approximately 16 percent of boys and girls of each age group strong deviations from the average indicators of physical development (within the norm) are observed, their fears become understandable.” According to I.S. Kona, a teenager is “overwhelmed by a thirst for the norm,” while the age of early adolescence is characterized by disproportions and the absence of the norm.
Many teenagers don't like their appearance. In their opinion, he does not correspond to their ideas about masculinity and femininity. The cultural stereotype that a man should be taller and bigger than a woman makes many teenage boys suffer. The gender role of girls presupposes external attractiveness, so they pay more attention to their face, figure, and skin. Some of the girls, striving for slimness, abuse diets and fasting.
Teenagers are concerned about many issues related to their physical self. Why do I have acne? Why am I short? Why don't I have strength (muscle mass)?
I -social. Adolescence is characterized by the fact that boys and girls “enter” a new social role. Previously, they were followers, but now they want more independence. Teenagers realize that they are not yet adults, but they are no longer children. They are driven by a “sense of adulthood,” a desire to assert themselves and “throw off the shackles of a child.”
In early adolescence, many teenagers become critical of their parents. Their example is no longer perceived absolutely, as in childhood, since the ideals of a teenager are not only found in the immediate environment. Many parents continue to treat teenagers like children. Naturally, this gives rise to conflicts and tension in relations with them. For the same reason, high school students often conflict with teachers at school.
Modern older teenagers have a negative attitude towards adults also because many adults cannot teach a teenager to live in modern conditions. The fact is that the skills and values of many teachers and parents are not aligned with “times of change.”
Thus, for a significant part of adolescents, the process of acquiring a new social status causes internal anxieties and tensions.
I'm sexy. During adolescence, puberty occurs. At this time, the teenager is identified as a carrier of either gender. E.I. Lebedeva notes: “One of the very important aspects“maturing” of the body is an aggravation of sexual problems: when the body has already acquired adult sexuality, but neither personally nor socially the teenager is yet ready for this. These problems feed the teenager’s already high emotionality.”
The above contradictions are aggravated by the fact that boys experience a period of hypersexuality during their early adolescence. Boys, and even some girls, have a lot of problems: how to make acquaintances, how to interact with the other sex, how to behave on a date. There is a lot of anxiety and difficulty here, especially against the backdrop of not always developed communication skills. Difficulties in intersexual relationships and the associated psychological discomfort give rise to anxiety and behavioral deviations.
I -psychological. Early adolescence is characterized by the discovery of the inner world and awareness of the reality of the “I”. According to I.S. Kohn that the development of self-awareness is a central mental process of adolescence.
The discovery of one's inner world directs the teenager's consciousness towards himself. This is manifested in an increased need to know oneself and, through this, in an increased interest in how he (the teenager) is perceived by others.
The formation of self-awareness raises a lot of questions among teenagers. Who am I? What's inside of me? Am I normal? Our experience of practical work with older adolescents allows us to state that the age of early adolescence is distinguished by a “thirst for knowing oneself.” In other words, the task of self-knowledge is very significant for older adolescents.
So, deviant behavior “drives” adolescents when their basic needs listed above are not satisfied. Unfortunately, modern society and schools cannot fully meet the basic needs of adolescents. Taking a surfactant (toxicant, alcohol or drug) satisfies these needs simultaneously.
How are the basic needs of adolescents satisfied after using psychoactive substances?
Physical-I. The “body” doesn’t bother me anymore.
Social-I. I am cool". In my peer group I am accepted as an adult.
Sexual-I. While “high” it is no longer difficult to communicate with the opposite sex and internal prohibitions on the expression of sexuality are lifted.
Psychological-I. The surfactant creates euphoria. Anxiety and tension are relieved.
It is naive to believe that just an explanation of how harmful surfactants are to health is enough for teenagers. For a teenager whose basic needs are not met, knowledge about the dangers of psychoactive substances is of little significance.
From the standpoint of the EP concept, preventive training and education should focus on developing students’ skills. And most importantly, schools and additional education systems should develop and implement systems of educational activities that could satisfy the basic needs of adolescents.
Awareness of adolescents and young people about drugs is one of the prerequisites for initiation into their use. To measure the actual scale of involvement, the indicator of the frequency of drug use among adolescents and young people was used. This indicator includes the first sample, which in the end may turn out to be the only one, but may also have a continuation; more frequent “samples”, which creates the preconditions for active consumption; regular consumption at relatively long intervals; regular consumption (every other day or daily), which means a strong drug addiction has developed.
Rice. 1
According to monitoring data, today 13.1% of children, adolescents and young people aged 11-24 use drugs. This is approximately 4 million people. This group includes those who consume drugs with varying frequencies - from 2-3 times a month to daily consumption.
Apparently, it is right to consider those 3.9% of those surveyed as drug addicts who resort to drugs daily or 2-3 times a week. This is both a total indicator of actual and potential drug addicts. To more or less accurately determine their number (with an error of ± 10%), you can use a number of empirical indicators.
According to monitoring data, among adolescents and young people aged 11-24 years, 803 thousand people were treated for drug addiction (2.5% of the total number of the surveyed category). According to our own estimates, 321 thousand people were cured. 482 thousand people believe that they have not been cured. To these should be added 418 thousand people who have not previously been treated, but believe that they need treatment (1.3% of the total number of those examined). It is also necessary to take into account 2 thousand military personnel (mostly conscripts), and 32 thousand people (0.1% of the total number of those surveyed) who are in a state of drug addiction (use drugs daily or every other day), but were not taken into account in previous indicators. The amount is 934 thousand people.
Based on the calculations made and using data from the State Statistics Committee of Russia, it is possible to determine the approximate number of drug addicts among the entire population (according to the State Statistics Committee, the proportion of drug addicts under the age of 25 is approximately 60% of the total number of drug addicts). According to extrapolation, among the entire population of Russia today there are approximately 1 million 557 thousand drug addicts. To this figure should be added 102 thousand drug addicts who are in institutions of the penitentiary system. The result is 1 million 659 thousand people.
Naturally, a number of categories of drug addicts are not taken into account in our calculations either due to the lack of statistical information or due to lack of monitoring (for example, patients undergoing dispensary treatment for drug addiction or other diseases who use narcotic drugs).
Based on monitoring data from the State Statistics Committee of Russia, departmental statistics, and also taking into account a possible correction due to the presence of some unaccounted for contingent, we can draw the following conclusion:
1) among children, adolescents and young people aged 11-24 years, today there are from 900 thousand to 1 million 100 thousand drug addicts.
2) this figure for the entire population of Russia ranges from 1 million 500 thousand to 1 million 800 thousand people.
The territorial scale of drug use by adolescents and young people is large. The epidemic is primarily affecting the European part of Russia, as well as the North and the Urals.
By retrospective extrapolation, based on monitoring data, the dynamics of the average age at which adolescents and young people began to engage in the use of psychoactive substances over the past 10 years was identified. As a result, the following indicators of the average age of initiation into the consumption of tobacco products, alcoholic beverages, and drugs were obtained.
Table 1
|
Average initial age of initiation into consumption: |
|||
|
Tobacco products |
Alcoholic drinks |
Narcotic drugs |
|
Judging by the table data, over the past 10 years, the average age at which adolescents and young people began mass consumption of tobacco products decreased by 3.5 years, alcoholic beverages - by 2.7 years, and narcotic drugs - by 3.7 years. In other words, since 1997 in Russian society The new “market” generation is becoming statistically significant, breaking the usual ideas about moral traditions Soviet period, identifying the principles of democracy with individualism and moral freedom. It's about the making of a generation western type, and in terms of consumption of psychoactive substances it is far from the best example. Thus, in Russia they began to register drug addicts at the ages of 7, 8 and 9 years. Increasingly, students are dying from drug overdoses. For example, in 2002 in St. Petersburg, a 15-year-old student, after injecting himself with heroin in the toilet, died right during class.
The highest proportion of drug addicts is among students in primary schools. vocational education(vocational school). It is 5 times higher than among school students, and 2.5 times higher than among students of technical schools and universities.
In Moscow and St. Petersburg, police are increasingly uncovering criminal groups of drug dealers selling deadly potions in educational institutions. The consumption of narcotic drugs is associated with the urbanization of the environment. Among adolescents and young people, the share of drug users in megacities is 2 times higher than in rural areas. Village youth traditionally prefer alcoholic drinks, mainly strong ones, including moonshine.
An average of 1,550 rubles per month or 18,600 rubles per year is spent per person aged 11-24 who are addicted to drugs. This amount is enough to purchase approximately 120-125 retail doses of narcotic drugs, with an average cost of one dose of 150 rubles.
Monitoring data makes it possible to calculate the approximate volume of drugs consumed per year (without taking into account the sample), as well as the amount of money spent on them. In 2002, Russians consumed approximately 695 million retail doses of narcotic drugs, totaling 130 billion 290 million rubles, or 4 billion 136 million US dollars.
Monthly expenses are on average: for those who consume 2-3 times a month - 700 rubles; for those who consume at least 2-3 times a week - 3,700 rubles.
Youth spending on drugs is high in the European part of Russia, the North, Eastern Siberia and the Far East.

Rice. 2
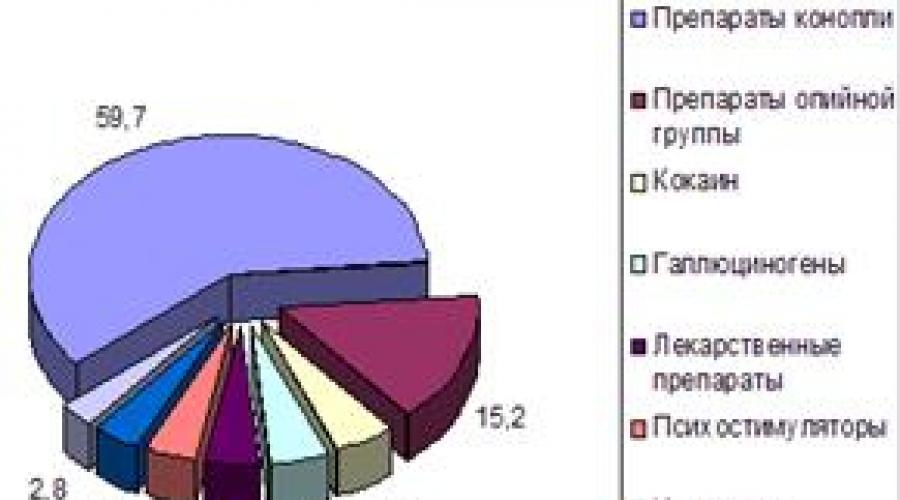
According to the official criterion adopted by the Main Directorate for Combating Smuggling of the Russian Customs Service, the cost of one retail dose of the drug averages 30 rubles. According to monitoring data, such a dose is sold at retail for an average of 150 rubles, resulting in the average potential profit of drug dealers retail network is at least 500%. Therefore, even with large losses of the drug mafia due to arrests and seizures of large quantities of drugs law enforcement agencies Russia, the profitability of the Russian drug market is high. Adolescents and young adults primarily consume cannabis preparations.
Among those who started using drugs of the opium group, every fourth switched to cannabis drugs, some - to psychostimulants.
Among those who started using hallucinogens, a sixth moved on to drugs of the opium group and medications.
Among those who started using psychostimulants, 50% switched to cannabis preparations and every tenth switched to medicinal preparations.
Among those who started using inhalants, half switched to cannabis preparations, a fifth - to medicinal preparations, and every tenth - to drugs of the opium group.
Among those who started with the use of drugs, a sixth moved on to drugs of the opium group.
The most consistent use is of cannabis and opium drugs. According to the respondents, the main reasons for preferring one drug or another are the following: for company, easier to get, less harmful to the body, cheaper, gives more pleasure.
Alcohol causes more harm to human health and society as a whole than heroin or crack. The findings of the study, published in the journal Lancet, call into question existing priorities in the fight against social evils.
Text: Alevtina Ivanova
Neuropharmacologist David Nutt from Imperial College London and his colleagues classified 20 harmful substances according to 16 parameters: nine of them assessed the harm caused to the person using these substances, and the other seven parameters assessed the harm caused to the people around him.
According to a specially developed scale, which experts, not without irony, called “the Independent Scientific Committee on Drugs” (ICSD), each substance received a certain number of points - from zero (harmless) to 100 (maximum harm). Points were awarded to the substance for the degree of addiction, for harm to mental and physical health“user”, as well as for the number of crimes, for material damage to the economy and society associated with its use.
Alcohol is 10 times more dangerous than LSD
As it turned out, the greatest harm to individual health is caused by the use of heroin, crack and methamphetamines. Alcohol, heroin and crack lead the way in terms of harm to others.
When the experts added up the scores for all parameters - both for individual and social harm - alcohol took the lead by a wide margin. He dialed maximum amount points - 72. The bottom line of the rating was occupied by hallucinogenic mushrooms, receiving only 5 points.
Another interesting discovery is that tobacco and cocaine scored the same number of points for harm to health and society. Although, individually, cigarettes turned out to be more harmful than cocaine.
 And in a completely unexpected turn - in the top three safe drugs included LSD, which in Russia belongs to the most dangerous category - List 1 of the List of narcotic drugs and psychotropic substances, the circulation of which is prohibited in the Russian Federation. According to experts, LSD is 10 times less harmful than alcohol sold on every corner.
And in a completely unexpected turn - in the top three safe drugs included LSD, which in Russia belongs to the most dangerous category - List 1 of the List of narcotic drugs and psychotropic substances, the circulation of which is prohibited in the Russian Federation. According to experts, LSD is 10 times less harmful than alcohol sold on every corner.
What evil to fight?
The study's findings contradict the official message about the dangers of alcohol and drugs adopted by the governments of most countries. Although the authors of the study themselves claim that their classification method, based on the consensus of several experts, provides a sufficiently accurate assessment that the authorities can use.
“Our findings support past studies conducted in Britain and Holland, which confirmed that modern systems classifications have little to do with the harm that different types of drugs cause,” the BBC Russian Service quotes Professor Nutt and his colleagues. Experts say the study's findings are consistent with previous expert reports suggesting that an aggressive crackdown on alcohol is the smartest and most necessary strategy.
By the way, defending such an approach at one time became the reason for the resignation of David Nutt from the post of head of the Drug Enforcement Council, a body whose conclusions influence the British government’s policy towards narcotic substances. A year ago, Professor Nutt was scandalously fired for disagreeing with the government's decision to change the country's existing drug classification, which serves as the basis for the fight against drug trafficking. In particular, Nutt was criticized by the transfer of marijuana from category C to category B, which meant tougher penalties for possession and sale of this substance. Increasing penalties for soft drugs is inappropriate and will only increase the burden on the police and the budget, Nutt argued.
Sociologists, doctors, psychologists, representatives of law enforcement, forecasting the development of drug addiction among children and adolescents for the next three to five years, note the dynamics of its growth and the strengthening of the following trend: further rejuvenation of the population using narcotic, potent and psychotropic substances.
The reasons for this phenomenon are also named. These primarily include the general deterioration of the socio-economic situation in the country, the growth of unemployment among young people, the growth of child homelessness and social orphanhood and a significant increase in the interest of the international drug mafia in the Russian market, which is focused on “promoting” the consumer demand of our youth.
The most significant reasons for the use of psychotropic substances are social difficulties in the family, school, and in conditions of unorganized free time. The use of any psychotropic substance at first cannot be called pleasant - nausea, vomiting, dizziness, pallor, poor general health. However, the proposing “senior comrades” regard this as a necessary element of joining the chosen ones. After the second or third use, there is still no craving, but each time the body reacts with irritability, poor sleep and appetite, and violations of normal social rules. The student misses classes, becomes undisciplined, withdrawn and gloomy.
The most common classification of reasons influencing drug use by children and adolescents includes the following reasons: : socio-economic, constitutional-biological, social, individual-psychological.
The socio-economic group of reasons is divided into two subgroups : global and traditional reasons.
To reasons of a global nature include the integration of our country into the world market system with all the ensuing consequences.
Traditional reasons - These are reasons peculiar only to our country, its individual regions, layers and groups of the population. An example is those groups of the population whose entire way of life was destroyed due to hostilities in the area where they lived, which resulted in their transition to the category of refugees. This entails the appearance of a maladaptation syndrome, which creates positive preconditions for the drug addiction of this part of the population. The traditional reasons that influenced the surge of interest in drugs in our country, and primarily, as we have already noted, among young people, were the long-existing prohibitive and punitive mechanism of action of various social institutions in relation to drug users.
Traditional reasons include the tolerant attitude that has developed in our country among the population towards such phenomena as alcoholism and smoking. Russia has always been considered a country of traditional alcohol consumption. In our society, there are a number of cultural stereotypes of alcohol consumption (regarding solemn, joyful and sad events). It cannot be said that everyone who drinks alcohol or smokes will become a drug addict. But the likelihood of such a transition is much higher for this category than for those who have a negative attitude towards alcohol and smoking.
Causes of a constitutional-biological nature usually include hereditary burden with mental or drug addiction diseases.
Social reasons are the influence on children and adolescents of the family environment, the reference group, and the social environment in general, including the enormous influence of the media and the success or failure of the child’s adaptation to an educational institution.
Reasons of an individual psychological nature usually include:
Imitating older teenagers or authoritative peers;
Attempts to neutralize negative emotional experiences;
The desire to fit in with the peer group that is significant for the teenager;
Abnormal personality traits (hedonism, adventurism, excitability, high or low self-esteem, increased conformity, instability of character);
“protest” reactions (“out of spite”) directed against elders (parents, teachers);
Self-destructive behavior;
Curiosity;
Submission to pressure and threats.
Factors associated with a greater susceptibility to drug use are called risk factors, and those associated with a reduced susceptibility to drug abuse are called protective factors.
There are many risk factors for drug abuse, each of which poses a threat to a person's psychological and social development and has different effects on him depending on the age phase. Affecting early development child family factors, are perhaps the most dangerous. These factors may be:
Unsupportive family environment, especially if parents abuse medications or suffer from mental illness;
Inept upbringing, which is especially dangerous for children with difficult characters and unbalanced behavior;
Lack of mutual understanding in the family and care for children on the part of parents.
Other risk factors relate to children's interactions with social entities outside the family (school, peers and community). Here are some of these factors:
Excessively timid or aggressive behavior in class;
Failed participation in school activities;
Inability to cope with social tasks;
Belonging to the “rejected” or those who are in contact with “rejected” children;
Positive attitude towards the behavior of substance abusers at school, among peers and in society.
There is also a group of protective factors that are not always completely opposite to risk factors. Their influence is also uneven in the development process. The most characteristic protective factors include:
Strong family ties;
A situation where parents monitor their children, are constantly involved in their lives and teach them clear rules of behavior within the family;
Success in school activities;
Strong connections to social institutions - for example, family, school, religious communities;
Compliance by others with generally accepted norms in the use of psychoactive substances.
Other factors, such as the availability of drugs, the nature of the drug trade and the belief that drug use is generally not unacceptable, also influence the number of young people who start using drugs.
The widespread prevalence of drug addiction is largely a consequence of the social conditions that exist there, namely: unemployment, uncertainty about the future, daily stress, a severe neuropsychic state, the desire to get doping, which creates the impression of a surge of strength, to escape at least for a short period of time. from the surrounding reality.
There are many theories that one way or another explain the causes of drug addiction:
1. the psychoactive substance has become a necessary component of metabolism;
2. a number of psychoactive substances are not foreign to the body, because in small doses they are produced by various cells and tissues (alcohol, opiates);
3. Social psychology at the basis of drug addiction sees the remnants of archaic thinking and the associated psychological attitude, which creates illusions of security and psychological comfort. In its modern form, these are toasts to health, success, various rituals for anniversaries, important events, subconsciously addressed to faith in obscure forces that can protect or ensure success.
Drug addiction among children and adolescents is of particular importance in modern social conditions. Children aged 12-13 years often find themselves in the “ranks” of drug addicts. The lot of the younger generation is non-alcoholic psychotropic substances. These include non-narcotic drugs (tranquilizers, cyclodol, ephedrine, etc.), household chemicals. They are easily available and cheap.
Of particular concern is the sharp “rejuvenation” of the population of drug addicts. Therefore, it is important to identify a teenager’s propensity for drug addiction and its prevention at that stage, until the additive behavior manifested in episodic drug use takes the form of a disease.
Thus, the causes of drug addiction primarily include the general deterioration of the socio-economic situation in the country, growth of unemployment among youth, growth of child homelessness, social orphanhood and a significant increase in the interest of the international drug mafia in the Russian market. It should also be noted that the psychological characteristics of a teenager’s personality - the risk of social maladaptation, a tendency to depression, the possibility and nature of suicide, alcoholism - are a risk of starting to use drugs, which is also the reason for the teenager’s tendency to drug addiction.