Motor function of the gastrointestinal tract. Motor function of the stomach Functions of the stomach physiology
Read also
functional activity all organs of the gastrointestinal tract (digestive system) and the stomach, in particular - motility, secretion and absorption, are regulated by a system of complex nervous and humoral mechanisms and are closely interconnected. The basis of the mechanism of regulation of the functions of the stomach is self-regulation and self-organization of the cells of its tissues. Coordination of the activity of the stomach and other organs of the digestive system is carried out through four interrelated components:
- nervous system - central and local;
- endogenous biologically active compounds that perform an informative (signal) and regulatory (corrective) role;
- microcirculation;
- the immune system.
Depending on location and nature regulatory mechanisms of organs digestion conditionally they can be divided into three groups:
- central reflex - conditioned reflex and unconditional reflex;
- humoral and
- local (local):
- nervous and
- paracrine.
The role of these groups in different parts of the digestive tract is not the same. In the initial sections (stomach and duodenum), reflex central mechanisms have a great influence, while as they move away from the oral cavity, their effect decreases, and the role of humoral factors increases. The activity of the distal small intestine and large intestine is mainly regulated by local factors that activate or inhibit the effects of mechanical and chemical irritations by the advancing food bolus and hormones of the APUD system.
Chyme has a stimulating effect on the secretion and motility of the digestive apparatus directly at its location and in the distal (caudal) direction, in the proximal (cranial) - depressing (inhibiting). But it must be emphasized that the leading and controlling role of the functional state of all organs of the digestive system belongs to certain structures of the brain, which is carried out with the help of unconditional reflex interactions. Chemo-, mechano- and thermoreceptors are located in the stomach, from which "information" through the afferent fibers of the vagus nerves enters the brain.
In the mucosa lining of the stomach allocate:
- mechanoreceptors - quickly and slowly adapting;
- chemoreceptors interacting with peptides, serotonin, dopamine, etc.;
- thermoreceptors - selectively "tuned" to thermal and cold stimuli;
- osmoreceptors that respond to changes in the osmolarity of the contents of the stomach;
- polymodal receptors that respond to various influences.
At present, more than 70 factors involved in the regulation of the digestion process, between which about 400 interactions have been established. However, if you use the formula that describes Newton's binomial, then the last figure will be many times larger.
Much is still unknown, and at present even mathematical models are created, with the help of which it will be possible to study in more detail the mechanisms of regulation of the process of digestion in dynamics, as well as to evaluate the influence of pharmacological substances. Therefore, when describing the basic physiological functions of the stomach, we will focus only on the action of the main factors that affect this organ.
Main physiological functions of the stomach are:
- reservoir function (accumulation of food mass) - food is retained in the stomach for 2-10 hours (according to different authors), which is determined by:
- composition of food;
- digestive activity of gastric juice;
- a person's way of life;
- compliance with the rules of nutrition, etc.;
- regulation of the temperature of the food bolus that has entered the stomach - heating or cooling;
- motor (motor) function - mixing and promoting food, and later chyme, through the digestive tract;
Mechanical processing of food is closely related to the motor function - mixing, grinding and dilution with mucus and gastric juice to form chyme;
- the leading function is the breakdown (digestion) of food ingredients (exocrine and endocrine activity of the stomach is closely related to this and other functions):
- denaturation (change in tertiary and/or quaternary structure) and chemical breakdown of proteins under the influence of hydrochloric acid (HCl);
- cleavage of proteins with the participation of proteolytic enzymes;
- enzymatic - the breakdown of fats under the influence of gastric lipase;
- hydrolysis of carbohydrates with the participation of carbonic anhydrases (amylase and maltase) of saliva;
- isolation of food, and later chyme, from other parts of the gastrointestinal tract (esophagus and duodenum) due to the presence of sphincters;
Sterilization of food mass (chyme) under the influence of hydrochloric acid and lysozyme;
- absorption (metabolic function) - water, salts, alcohol, monosaccharides, some drugs, etc.;
- exocrine secretory function - secretion of gastric juice ingredients:
- proenzymes and enzymes (secreted mainly by the chief cells) - propesinogen, which turns into pepsinogen and breaks down proteins to peptones;
- chymosin - is involved in the breakdown of proteins, mainly milk (casein), which is expressed in the curdling of milk;
- gastric lipase - breakdown of fats;
- lysozyme (bactericidal action) - splitting of bacterial membranes;
Hydrochloric acid (secretion of hydrogen and chlorine ions is carried out by parietal cells), which:
- leads to denaturation and swelling of proteins, which ensures greater availability of the protein molecule for the action of enzymes;
- activates propepsinogen with the formation of pepsinogen;
- has antibacterial action;
- regulates the secretion of mucus and enzymes, etc.;
- mucus - an insoluble fraction - covers the surface of the mucous membrane, isolates epithelial cells from the aggressive action of hydrochloric and digestive enzymes (mechanical and chemical protection);
- soluble fraction - forms a colloidal solution in which the components of gastric juice are dissolved;
It has buffer properties, i.e. maintains acidity at a certain level;
- anti-anemic factor (internal Castle factor) - synthesized by parietal cells; its presence is necessary for the absorption of vitamin B12 in the intestine, in its absence, anemia develops, the synthesis and secretion of the factor is stimulated by histamine, gastrin, and also increase when the vagus nerve is activated (acetylcholine);
- in the acidic environment of the stomach, iron ions are oxidized, which contributes to its absorption in the small intestine;
- sterilization of incoming food occurs in the acidic environment of the stomach;
Hormonal function - various endocrine cells synthesize biologically active compounds (gastrin, serotonin, motilin, etc.), which have endocrine, neuroendocrine and paracrine effects, and are involved in the regulation of secretory and motor activity;
- excretory function - excretion of ammonia, uric acid, urea, creatinine from the blood into the cavity of the stomach);
- formation of immune responses involved in the formation of antitumor immunity (mucosa);
- participation in the regulation of water-salt metabolism and acidity (pH) of the blood.
The stomach performs the function of a depot, where not only the hydrolysis of nutrients occurs, but also the accumulation of chyme - up to 3 l, which gradually passes into the duodenum from the pyloric region due to the propulsive contraction of its smooth muscles. The following stages of regulation of the motor function of the stomach can be distinguished:
1 "Receptive relaxation" of the stomach- in the case of food entering its cavity, the proximal part - the bottom and the body - relax, adapting the volume of the stomach to a slight increase in pressure. This is due to the weight-vagal reflex, because after the section of the vagus, relaxation does not occur. Cholecystokinin-pancreozymin (CCK-PZ) is also involved in receptive gastric relaxation and goaltender contraction.
2 Mixing of stomach contents is carried out due to the contraction of the muscles of its distal section as follows:
Slow waves of depolarization of smooth muscles occur with a frequency of 3-5 per 1 min. When the threshold value of depolarization is reached, APs are generated, which leads to muscle contraction (Fig. 13.20)
The wave of muscle contraction moves in the distal direction of the pyloric stomach - antral systole. In this case, the contents of the stomach slowly move with gastric juice. Following this, peristaltic waves (their amplitude and propagation speed) increase, as a result of which the chyme is pushed to the exit from the stomach;
Gastric contractions increase with vagus nerve activation and decrease with sympathetic activation.
3 Evacuation of contents from the stomach carried out by coordinated successive reflex contractions of the antral and pyloric sections, an increase in pressure in the pyloric section up to 10-25 cm of water. Art., opening the gatekeeper (pylorus), so that a portion of the chyme enters the duodenum 12. The contraction of the pyloric sphincter, which occurs after this under the influence of the local duodeno-gastric reflex, does not allow the chyme to return back.
The evacuation time of mixed food from the stomach is 6-10 hours.
Other factors also affect the speed of evacuation:
■ a positive pressure gradient between the stomach and the duodenum, sufficient for the passage of gastric contents,
■ fats move into the duodenum, suppress evacuation due to prolonged contraction of the pyloric sphincter under the influence of CCK-PZ secreted in it;
■ ions Η+, entering the duodenum with chyme, suppress evacuation by the mechanism of the local duodeno-gastric reflex, which leads to a contraction of the pyloric sphincter;
■ isotonic chyme is evacuated faster than hypertonic chyme.
Hungry stomach contractions occur every 90 minutes with an empty stomach, due to the pacemaker activity of myocytes, which form migratory motor complex(MMK) - cycles of motor activity migrating from the stomach to the distal ileum. In the stomach, such a pacemaker is located on the lesser curvature in the proximal part of its body. From here, the contraction spreads towards the pylorus, which contributes to its release from food debris. The main regulator of MMK is the hormone motilin- a polypeptide that is produced by ECL cells and Mo cells of the stomach. Its concentration increases 100 times in the intertraumatic period every 90-100 minutes. In case of introduction mo tilin there are contractions of the smooth muscles of the stomach and intestines.
RICE. 13.20. Balonographic registration of motor activity of the dog's stomach. I - hungry: A - period of physical activity; B - period of rest. II - peristaltic types of contractions of the fundic part of the stomach during food activity: 1 - weak; 2 - strong; 3 - tonic
The motor function of the gastrointestinal tract is based on the contractile activity of smooth muscle cells. They make up the smooth muscle layers of the alimentary canal. internal (circular), outer (longitudinal) and submucosal.
Conjugation of excitation with contraction. Characteristic properties of smooth muscle cells of the gastrointestinal tract are their automation and contraction response to stretch. Cellular automation manifests itself slow waves- rhythmic fluctuations in the membrane potential, which have a myogenic nature. At a critical level of membrane depolarization, action potentials, which is accompanied by cell contraction.
Activation of the contractile apparatus smooth muscle cells is carried out with the participation of Ca 2+ ions, which enter the cells through calcium channels. The result is a rapid phasic contraction of smooth muscle cells.
After the disappearance of the action potential, the contraction may continue, but it proceeds more slowly. This component of the contractile process occurs when there is a certain level of depolarization of the cell membrane. Slowly developing tonic cell contraction is characteristic of the functioning chemosensitive calcium channels opening under the action of biologically active substances, such as acetylcholine, in high concentrations.
The frequency of slow waves in each section of the digestive tube is fairly stable, but decreases in the direction from the duodenum to the ileum. There are several areas in the gastrointestinal tract that have a high frequency of slow waves. They perform functions pacemaker. In the intestine, one pacemaker zone is localized in the duodenum at the confluence of the bile and pancreatic ducts, the other in the ileum.
The greater the frequency and amplitude of action potentials, the stronger the reduction takes place. The frequency of phase contractions corresponds to the frequency of slow waves carrying action potentials. An increase in the frequency of slow waves in the presence of numerous action potentials on them leads to the appearance of a jagged or smooth tetanus.
The main types of motor activity of the gastrointestinal tract are peristaltic contractions and rhythmic segmentation. There are also pendulum movements. At peristalsis contraction of the circular muscle layer spreads along the digestive tube like a wave. Sufficiently strong peristaltic contractions move the chyme to the distally located sections of the gastrointestinal tract. Such movements are propulsive.
Rhythmic segmentation manifested by the simultaneous contraction of the circular muscle layer in neighboring sections of the intestine, as a result of which the latter is divided into segments. Rhythmic segmentation ensures the mixing of chyme. pendulum movements arise as a result of rhythmic contractions of the intestine, leading to the movement of chyme a short distance along the digestive tract and back. In the gastrointestinal tract there are sphincters (lower esophageal, pyloric, ileocecal and internal anal sphincters).
They are characterized by tonic contractions.Regulation of the contractile activity of the muscles of the gastrointestinal tract. Acetylcholine has a stimulating effect on the smooth muscles of the gastrointestinal tract. Adrenaline, norepinephrine cause inhibition of the contractile activity of the stomach and intestines as a result of the effect on inhibitory adrenoreceptors located on the membrane of smooth muscle cells. However, norepinephrine is able to cause contraction of the sphincters of the gastrointestinal tract.
Stretching of the intestinal tube causes the appearance or increase in the contractile activity of smooth muscles. This reaction reflects the manifestation of the peristaltic reflex, which closes in the ganglia of the enteric plexus. With this reflex, a propulsive contraction of the circular layer of muscles occurs with relaxation of the longitudinal one.
With mechanical irritation of the intestine, inhibition of contractile activity below the site of irritation may occur. Here, probably, the mechanism of non-adrenergic non-cholinergic inhibition is involved.
Reflexes that are realized with the participation of estramural innervation take part in the regulation of the activity of the muscles of the gastrointestinal tract. A number of biologically active substances are able to influence the contractile activity of the smooth muscles of the gastrointestinal tract. Their effect depends on the site of action and the functional state of smooth muscles.
Exciting effect on the contractile activity of the stomach and small intestine has motilin. Cholecystokinin inhibits contraction of the fundus and stimulates the activity of the antrum. The same effect causes gastrin. enkephalins, inhibiting the motility of the stomach and small intestine, have a stimulating effect on the smooth muscles of the colon and cause contraction of the pyloric sphincter. Somatostatin, vasoactive intestinal peptide and gastroinhibitory peptide have an inhibitory effect on the smooth muscles of the stomach and small intestine.
Motor function of various parts of the gastrointestinal tract. After entering the oral cavity, solid food is exposed to chewing. The chewing process is a strictly coordinated activity of the masticatory muscles, tongue, cheeks and soft palate. With movements of the tongue and cheeks, food is placed in the space between two rows of teeth, cut and rubbed by them. The food bolus formed as a result of chewing is swallowed.
swallowing- a reflex act that occurs as a result of irritation of the sensitive endings of the soft palate, the base of the tongue and the back wall of the pharynx by the food lump. To the center of the swallowing reflex, located at the bottom of the IV ventricle of the medulla oblongata, excitation comes through the glossopharyngeal nerves. Efferent impulses from the medulla oblongata travel along the hypoglossal, trigeminal, glossopharyngeal, and vagus nerves.
There are three phases in the act of swallowing: oral(arbitrary), pharyngeal(fast involuntary) and esophageal(slow involuntary). When swallowing, the entrance to the larynx is closed, which prevents food from entering the respiratory tract.
Promotion of the food bolus through the esophagus is provided by a peristaltic wave of contraction of the circular muscles, which advances the food bolus to the cardial part of the stomach. The wave of relaxation causes a decrease in the tone of the esophageal sphincter, and the wave of contraction transfers the food bolus into the stomach.
Food from the esophagus enters the fundus of the stomach. This results in smooth muscle relaxation.
This process is referred to as receptive relaxation(perceiving relaxation). Due to this reaction and the plasticity of the muscles of the stomach, even when a large amount of food enters the stomach, the pressure in it changes only to a small extent. Reservoir and digestive functions are carried out by the bottom and body of the stomach, and the evacuation function is realized mainly by the antrum.Stirring and promotion of stomach contents carried out by peristaltic waves that occur on the greater curvature in the area adjacent to the esophagus. A peristaltic wave traveling through the body of the stomach moves a small amount of chyme into the antrum, which is adjacent directly to the mucous membrane and is most exposed to the digestive action of gastric juice.
Most of the peristaltic waves are damped in the antrum, however, some of them propagate there with increasing amplitude, which leads to pronounced peristaltic contractions of this section, an increase in pressure and the opening of the pyloric canal. In this case, part of the contents of the stomach passes into the duodenum, but a significant part moves back to the proximal part of the antrum, resulting in a grinding effect.
Gastric emptying occurs as a result of the interaction of the contractile activity of the body of the stomach, its antrum, pyloric sphincter and duodenum. The emptying of the stomach after a mixed meal occurs at first quickly, then more and more slowly.
AT regulation of the evacuation function of the stomach the enterogastric reflex takes part, which causes inhibition of the contractile activity of the stomach when chyme enters the duodenum. Under the action of fats and hydrochloric acid on the duodenal mucosa, secretin and a gastroinhibiting peptide are released, which also have an inhibitory effect on the contractile activity of the stomach. Gastric emptying is inhibited by enkephalins.
AT regulation of small and large intestine motility activating reflexes that occur when the esophagus and stomach are stretched take part. Gastrin, motilin and cholecystokinin stimulate, while secretin, intense vasoactive peptide and gastroinhibitory peptide inhibit the motor activity of the small intestine.
A feature of the motility of the large intestine is the presence in it of antiperistalsis. Slow peristalsis and antiperistalsis, as well as rhythmic segmentation, ensure the mixing of the contents of the colon. Propulsive peristalsis is manifested by waves of strong contractions that move the contents of the intestine into its distal sections and into the rectum. excretion, formed in the large intestine, is carried out during the act defecation. The urge to defecate occurs as a result of distension of the rectum by stool.
Periodic motor activity of the gastrointestinal tract. The study of periodic motor activity of the intestine led to the emergence of the concept migrating myoelectric (motor) complex. When registering the contractile activity of the intestine, the appearance of short (3-7 min) periods is noted, which consist of contractions that occur with a maximum frequency. Such periods are repeated after approximately 90 minutes. When registering motor activity in several parts of the intestine, a slow movement of the frontal activity from the duodenum or the proximal part of the jejunum to the terminal part of the ileum is noted within 90-120 minutes. Eating eliminates the migrating myoelectric complex in all parts of the small intestine. Instead, there is constant contractile activity.
The periodic motor activity of the gastrointestinal tract is due to the joint functioning of peripheral and central nervous mechanisms and humoral regulators. Somatostatin is involved in the formation of periodic contractile activity of the gastrointestinal tract, without being mandatory for its occurrence. Motilin causes the appearance of frontal activity in the upper intestines.
Intermittent intense activity clears the digestive tract of chyme residues and discarded epithelial cells between meals and prevents the spread of microflora up the small intestine.
Literature
Atlas of Normal Physiology / Ed. A.V. Korobkova, S.A. Chesnokova. - M .: Higher School, 1986.2. General course of human and animal physiology / Ed. A.D. Nozdrachev. - M .: Higher School, 1991.
3. Fundamentals of human physiology / Ed. B.I. Tkachenko. - St. Petersburg, 1994.
4. Human Physiology / Ed. V.M. Pokrovsky, G.F. Korotko. – M.: Medicine, 2000.
5. Human Physiology / Ed. R. Schmidt, G. Teus. In 3 volumes - M .: Mir, 1996.
6. Human and Animal Physiology, Ed. G.I. Kositsky. – M.: Medicine, 1985.
7. Physiology of man and animals / Ed. P.B.Kogan. - M .: Higher School, 1984.
For the full digestion of food in the gastrointestinal tract, it is necessary to grind it and process it with digestive juices. The motor function of the stomach is represented by various types of contractions, the coordinated work of which is controlled by the nervous system and the body's own impulses. If the regulation is impaired or there is a pathology of the gastrointestinal tract, there is a weak or excessive contractility. To normalize digestion, drugs that regulate motility, herbal decoctions and infusions, and a diet are used.
What is gastric motility?
The physiological process of contraction of the gastric muscles, which contributes to the mechanical and chemical processing of food for further passage to the intestines, is called motility. Wavy contractions of the smooth muscles of all parts of the stomach occur under the influence of reflexes, have different frequencies and are not controlled by consciousness. Healthy motor activity of the body contributes to the quality digestion of food in the lower sections of the gastrointestinal tract.
Types of abbreviations
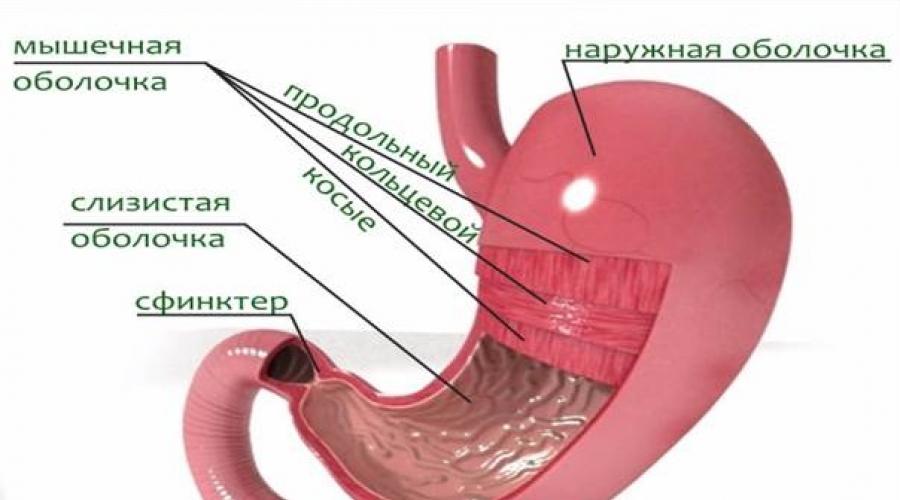
 The muscle layer consists of three types of muscles.
The muscle layer consists of three types of muscles. The muscular layer of the stomach consists of longitudinal, circular and oblique muscle fibers. Varieties of the motor activity of an organ are determined by the abbreviations of its departments. The bottom and body of the stomach are involved in grinding food, and the pylorus zone is involved in evacuation. Periodic spastic impulses occur at moments of lack of food. This phenomenon is called hungry motility.
Principle of contraction of the stomach
 The central nervous system plays an important role in the digestive system.
The central nervous system plays an important role in the digestive system. The physiology of the process is quite complex. The regulation of motility occurs with the participation of the nervous system, through reflexes and mechanical irritation of the receptors of the gastrointestinal tract, its own pacemakers, which are localized in the cardial and pyloric parts of the stomach and stimulate tone, as well as hormones. After ingestion of food, the muscles of the stomach relax and stretch for a while. An hour later, peristaltic contractions of the circular muscles begin, which grind, grind food and contribute to its comprehensive processing by digestive juices. After the formation of the slurry - chyme, the muscles of the antral zone periodically begin to actively work, which ensures portioned delivery of the food bolus into the cavity of the small intestine.
Most often, digestion slows down in people with an unhealthy diet and a disordered diet.
Causes of motor disorders
 Poor nutrition is the root cause of diseases of the digestive tract.
Poor nutrition is the root cause of diseases of the digestive tract. A failure in a well-coordinated system that carries out motor activity affects the work of the entire digestive tract. Violation of the motility of the stomach to provoke a local disease of the organ or systemic pathology of the gastrointestinal tract, dysfunction in the mechanisms of regulation of the process. A list of common reasons why there are difficulties with the motor function of the stomach:
- Organ pathologies:
- ulcers;
- tumors;
- scarring.
- Chronic diseases of the gastrointestinal tract:
- cholecystitis;
- pancreatitis;
- gastroesophageal reflux.
- Transferred operations.
- Age changes.
- Heredity.
- Constant nervous tension.
- Long courses of medications.
- Physical inactivity.
Symptoms of pathology
 Frequent vomiting and nausea after eating are possible.
Frequent vomiting and nausea after eating are possible. Poor motor activity of the stomach affects the well-being of a person. Contractile activity and muscle tone can increase or slow down, and the symptoms depend on this. If the muscles of the stomach are sluggish, the patient suffers from heaviness in the abdomen, a feeling of rapid satiety with a small amount eaten. And hyperkinesis leads to diarrhea. Also, the pathology can be manifested by the following symptoms:
- heartburn;
- nausea;
- vomit;
- abdominal pain;
- belching;
- bad breath;
- flatulence;
- constipation or diarrhea;
- insomnia, mood changes;
- weight gain or loss.
How is the treatment going?
 Timely diagnosis and treatment will help to avoid complications.
Timely diagnosis and treatment will help to avoid complications. To bring gastric motility back to normal, it is necessary to accurately determine the type of pathology. For this, you should contact a gastroenterologist. By the presence or absence of certain symptoms, the doctor may suspect the type of pathology. After an examination and an accurate diagnosis, the gastroenterologist will be able to decide on the direction of therapy. For treatment, medicines are used that enhance or slow down the motility of the stomach, folk herbal remedies, physiotherapy. A prerequisite for the treatment of any digestive diseases is diet.
Mechanical processing of food (grinding, mixing with digestive juices), as well as the movement of food, depend on the motor (motor) function of the gastrointestinal tract, that is, the rhythmic contractions of the walls of the digestive canal
The motor function of the gastrointestinal tract is composed of peristalsis and non-peristaltic movements.
Non-peristaltic movements in the oral cavity include sucking, chewing and swallowing.
Peristaltic, systolic and tonic contractions occur in the stomach
Peristaltic movements are carried out by contraction of the circular muscles of the stomach. The contraction wave begins in the region of the cardiac sphincter and extends to the pyloric sphincter. Peristaltic waves occur at a frequency of 3 times per 1 minute
Systolic movements (antral systole) are associated with contraction of the terminal part of the pyloric stomach. These movements ensure the transition of a significant part of the contents of the stomach into 12 pc
Tonic contractions are due to a change in the tone of the muscles of the stomach. An increase in muscle tone leads to a decrease in the volume of the stomach and an increase in pressure in it. The duration of tonic contractions is from one to several minutes. With a decrease in muscle tone, especially the fundus of the stomach, the volume of the organ increases and conditions are created for the intake of more food.
With an empty stomach, periodic contractions occur, followed by a period of rest. In humans, the duration of the work of the stomach is 20-50 minutes, rest -45-90 minutes or more. Periodic contractions of the stomach stop with the onset of eating and digestion
In addition to these types of contraction, antiperistalsis may occur in the stomach (during the act of vomiting)
Note that there are peristaltic and non-peristaltic movements in the small intestine.
Peristaltic contractions of the small intestine ensure the movement of food gruel through the intestines. This type of motor activity is due to a coordinated contraction of the longitudinal and circular layers of muscles: contraction of the annular muscles of the upper segment of the small intestine and squeezing out the food slurry into the lower section simultaneously expanding due to the contraction of the longitudinal muscles. A wave of peristaltic contractions runs along the entire intestine and promotes the movement of food gruel to the rectum
Non-peristaltic movements of the small intestine are represented by rhythmic segmentation and pendulum movements.
Rhythmic segmentation is provided by contractions of the circular muscles, as a result of which the resulting transverse intercepts divide the intestine into small segments. After a while, these transverse constrictions relax and reappear, but already in other parts of the intestine. Rhythmic contractions divide the food gruel into separate segments, which contributes to its better rubbing and is due to contraction of the circular and longitudinal muscles of the intestine. In a small area, as a result of successive contractions of the annular and of the longitudinal muscles, the segment of the intestine either shortens and expands at the same time, then lengthens and narrows. Successive changes in the diameter of the intestine and its length lead to the movement of the food gruel in one direction or the other, like a pendulum. Pendulum-like movements also contribute to a thorough mixing of chyme with digestive juices
Remember that peristaltic, antiperistaltic and pendulum movements are distinguished in the large intestine. All these types of motor activity, unlike those in the small intestine, are carried out slowly. Their significance is that they provide mixing, kneading the contents, contribute to its thickening and absorption water.
Peristaltic contractions of the large intestine are not of great importance in the promotion of its contents. The large intestine has a special type of contraction, which is called mass contraction (mass peristalsis). Mass peristalsis rarely occurs, up to 3-4 times a day. Contractions capture most of large intestine and provide rapid emptying of large sections of it
The motor function of the gastrointestinal tract in children in comparison with adults has some features. You need to know that the motor function of the stomach in young children is slow. However, they have well-defined hunger contractions, which often cause children to wake up
The motor function of the intestines in children is more energetic. Therefore, they have an act of defecation more often than adults
The motor function of the alimentary canal is regulated by nervous and humoral mechanisms.
Nervous regulation is provided by the intramural and extramural nervous system
The intramural nervous system is represented by local plexuses embedded in the wall of the gastrointestinal tract, the extramural nervous system is represented by fibers of the parasympathetic and sympathetic nervous system.
The parasympathetic nerves include: the vagus nerve that innervates the esophagus, stomach and small intestines, as well as the pelvic nerve that innervates the large intestine. These nerves increase the tone of the muscle wall, determine the motor function of the alimentary canal and at the same time lower the tone of the sphincters
The sympathetic nerves include: the celiac nerve that innervates the esophagus, stomach and small intestines and the hypogastric nerve that innervates the large intestines. These nerves lower the tone of the muscle wall, inhibit motility and increase the tone of the sphincters
Humoral regulation of motility is carried out by hormones of the gastrointestinal tract. Thus, the hormones gastrin, enterogastrin, motilin stimulate gastric motility, secretin and cholecystokinin-pancreozymin stimulate the motor function of the small intestine, enterogastron inhibits peristalsis
In addition, the hormone insulin stimulates the motility of the alimentary canal, and adrenaline inhibits it.
Biologically active substances such as histamine, serotonin, angiotensin, bradykinin, kallidin, some prostaglandins also stimulate the motor function of the gastrointestinal tract
http://trundel.ru/%D0%BC%D0%B5%D1%82%D0%BE%D0%B4%D0%B8%D1%87%D0%BA%D0%B8/%D1%84% D0%B8%D0%B7%D0%B8%D0%BE%D0%BB%D0%BE%D0%B3%D0%B8%D1%8F/%D0%BC%D0%BE%D1%82%D0 %BE%D1%80%D0%BD%D0%B0%D1%8F-%D1%84%D1%83%D0%BD%D0%BA%D1%86%D0%B8%D1%8F-%D0 %B6%D0%B5%D0%BB%D1%83%D0%B4%D0%BE%D1%87%D0%BD%D0%BE-%D0%BA%D0%B8%D1%88%D0% B5%D1%87%D0%BD%D0%BE%D0%B3.html